impact of Poverty on Health
| ✅ Paper Type: Free Essay | ✅ Subject: Health |
| ✅ Wordcount: 2840 words | ✅ Published: 16 Oct 2017 |
1
Health
Access to Nursing
Health
Assignment 2
Kirsty Lincoln
Tutor – Lis Footsoy

This should be in the report format! Please follow Assignment Brief instructions carefully!
According to Ogden (1996), there are many factors that impact on the health of individuals within society, some are more common than others such as poverty, unemployment, lifestyle and residential areas. Alongside these are medical factors, religion and differing beliefs in medicine and health. According to Ogden (1996) although these are all different areas to take into consideration they are all interlinked to one another and it is often thought that if an individual has any one of the above chances are they will have some degree of each one impacting on their general health and wellbeing.
 [LF1]Naidoo and Wills (2000) claim that there are many determinants also known as health inequalities, which can all be broken down into categories such as social, environmental, lifestyle and physiological factors, it can be suggested that social factors have a major impact on health and the way individuals live generally associating health with social class, lower working classes are seen to lead unhealthier lifestyles due to poverty or lack of employment which in effect will lead to poor housing and living in higher crime rate areas and less access to health services and very little means of leisure activity which will then result in poor nutrition as not many individuals in the lower classes can afford healthy food and 10 fresh fruit and vegetables a day which is needed to maintain a good level of health, this could also include high consumptions of alcohol and cigarettes. Naidoo and wills (2000) explains how all this then leads to physiological factors that impact on health like stress and depression, high blood pressure, heart disease and obesity which then ends up costing the National Health service thousands and thousands of pounds each year. It can be suggested that this is just a vicious cycle and until poverty and unemployment levels decrease, society as a whole will continue to consume money in the NHS.
[LF1]Naidoo and Wills (2000) claim that there are many determinants also known as health inequalities, which can all be broken down into categories such as social, environmental, lifestyle and physiological factors, it can be suggested that social factors have a major impact on health and the way individuals live generally associating health with social class, lower working classes are seen to lead unhealthier lifestyles due to poverty or lack of employment which in effect will lead to poor housing and living in higher crime rate areas and less access to health services and very little means of leisure activity which will then result in poor nutrition as not many individuals in the lower classes can afford healthy food and 10 fresh fruit and vegetables a day which is needed to maintain a good level of health, this could also include high consumptions of alcohol and cigarettes. Naidoo and wills (2000) explains how all this then leads to physiological factors that impact on health like stress and depression, high blood pressure, heart disease and obesity which then ends up costing the National Health service thousands and thousands of pounds each year. It can be suggested that this is just a vicious cycle and until poverty and unemployment levels decrease, society as a whole will continue to consume money in the NHS.

The graphs above shows the unemployment rates in the united kingdom compared to other countries, it is suggested that although it is not at the higher end of the scale there is still a high number of unemployment which has a major impact on the National Health service and the united kingdom’s economy which will in turn effect the overall health of the general public through poverty.
It is clear to see from this brief overview how all the determinants are interlinked and how each one individually affects health and wellbeing.
Ogden (1996) states that what is clear is that ill health does not happen by chance or through bad luck, in order to maintain health, society as a whole should promote it. The Lalorde report published in 1974 helped identify four fields of health that can be improved these are: Genetics and biological factors which determine an individual’s disposition to disease, lifestyles factors in which health behaviours contribute to illness, environmental factors like housing or pollution and the health services provided. If an area has a poor health service than it is more likely that death rates are higher through disease and health will be effected. These show that factors other than genetic and biological all affect an individual’s health but it is possible to change it.
Naidoo and w[LF2]ills (2000) explains that unemployment and low income is a major determinant of living standards and when studying levels of income and material deprivation through unemployment it has been found that it can tie in with ill health and premature mortality.

The graph above shows the different ages and class groups of the working environment it shows the level of deaths are a lot higher in those who work in manual hard labour which is very hands on and demanding in comparison to those of other intermediate and higher professional backgrounds paying in higher wages than other lower class jobs.
According to the Rowntree report in 1990, 24% of the population had an income of below the national average after allowing for housing costs (Rowntree foundation 1995), people most likely to be in this category are the unemployed, pensioners, lone parents and the low paid. Blackburn suggests that there are three ways in which low income and unemployment can affect health, Physiologically – inadequate housing, lack of warmth, lack of food, psychological – stress lack of support network and behavioural – health damaging behaviours like excessive smoking, drinking alcohol, sweets for children instead of healthy foods, living in poverty can affect anyone and without the means to provide a healthy lifestyle many are forced to live unhealthy lifestyles to make ends meet, it is not a choice.
 According to Ogden (1996) one of the main challenges the National Health Service (NHS) has to deal with is the constant usage of money, as healthcare costs thousands each year and regions with poor housing and less deprived areas spend more due to leading unhealthy lifestyles, an issue with this is that those people who are unemployed who live in these poorer communities pay nothing into the system yet can still access healthcare with the same rights as people employed who do pay into the system and pay taxes, so people who are unemployed can claim benefits, healthcare should be free and accessible to everyone although there will come a time when there is no financial funding left to pay for healthcare, there have been suggestions of placing a charge for every time the individual visits the doctor or attends Accident and Emergency on a Friday night when they have been found too intoxicated to function. This in turn will promote a healthier living although it can be seen as discrimination as individuals in poverty or unemployment still will not have the means to pay for the healthcare visits resulting in poor health and diseases increasing, having a detrimental effect on the health and wellbeing within society.
According to Ogden (1996) one of the main challenges the National Health Service (NHS) has to deal with is the constant usage of money, as healthcare costs thousands each year and regions with poor housing and less deprived areas spend more due to leading unhealthy lifestyles, an issue with this is that those people who are unemployed who live in these poorer communities pay nothing into the system yet can still access healthcare with the same rights as people employed who do pay into the system and pay taxes, so people who are unemployed can claim benefits, healthcare should be free and accessible to everyone although there will come a time when there is no financial funding left to pay for healthcare, there have been suggestions of placing a charge for every time the individual visits the doctor or attends Accident and Emergency on a Friday night when they have been found too intoxicated to function. This in turn will promote a healthier living although it can be seen as discrimination as individuals in poverty or unemployment still will not have the means to pay for the healthcare visits resulting in poor health and diseases increasing, having a detrimental effect on the health and wellbeing within society.
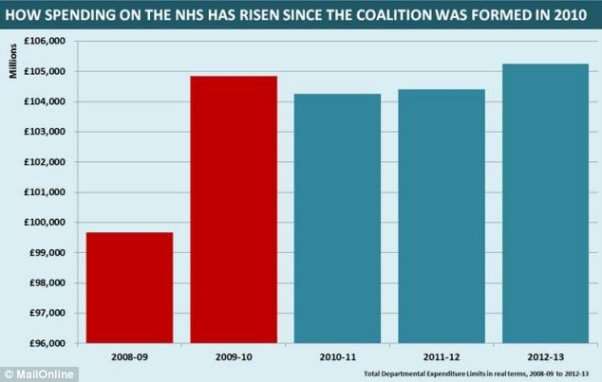
The graph above shows how the National Health Service funding has increased over the last 7 years reaching a high of just over £105,000 in the years 2012 to 2013.
As Naidoo and wills (2000) explains there are some factors that impact health that we cannot change for example: ethnicity, different race and ethnic backgrounds can determine an individual’s health for example: individuals with darker skin have a higher protection from diseases of the skin, caused by sunlight such as skin cancer and individuals with lighter more pale skin can burn easily and be allergic to the sun, this can tie into the environmental factors that affect health. Although in order to fit in to society in modern day it can be seen that there is a lot more pressure placed on young girls and women who feel the need to be perfect due to the mass media resulting in a rise in the use of tanning beds in order to gain a tan and darkening of the skin, this heightens the chance of skin cancer and other skin diseases.
The graph below shows that in 2010, among men, white men had the highest rate of getting melanoma of the skin, followed by American Indian/Alaska Native, Hispanic, Asian/Pacific Islander, and black men. Among women, white women had the highest rate of getting melanoma of the skin, followed by Hispanic, American Indian/Alaska Native, Asian/Pacific Islander, and black women.
 Melanoma of the Skin Incidence Rates* by Race/Ethnicity and Sex, U.S., 1999–2010
Melanoma of the Skin Incidence Rates* by Race/Ethnicity and Sex, U.S., 1999–2010
It can be suggested that along with this, studies have found to show that younger people particularly are at risk using a tanning bed as people who start using sunbeds before the age of 35 are 87% more likely to develop Melanoma compared to people with darker skin from different ethnic groups or those who never use sun beds. [LF3]
It can also be said that on the other hand certain ethnic groups are more prone to specific diseases, darker skin is especially prone to sickle cell disease, and individuals who are prone to certain diseases can use the National Health Service at their discretion depending on their beliefs surrounding medicine. Although in some countries like America, certain ethnic groups do not believe in the health care system American Indians believe disease is an act of nature and should be allowed to follow its course. It can also be said that in third world countries medicine and healthcare is not easily accessible as there is little funding to provide the adequate care. It can also be suggested that some regions with less sunlight can also affect health due to causing psychological factors like stress and Seasonal Affected Disorder (SAD) which is a disorder affected by seasons which in turn causes higher suicide rates in winter colder months in comparison to summer months.
It is possible that all things in society affect health and although looking at this from a Marxist point of view unemployment and poverty are a root cause to most health issues. Marxists believe that everyone should be equal and that poverty helps maintain the domination of the Bourgeoisie (upper class) it serves the interest of the wealthy, although other sociologists disagree and argue that individuals are to blame for their own poverty or as groups they develop a culture of poverty. Marxists believe poverty is rooted to the structure of society rather than a specific individual therefore if an individual lives in a deprived area they are more likely going to adapt to the ways of that community leading to ill health through poor lifestyles. [LF4]
Along with Karl Marx another sociologist Charles Murray (1989) [LF5]stated that poverty is caused by the lower class in the sense that the lower class do not want to work or find employment, he blames illegitimacy for this state of poverty in 1979 Britain had an illegitimacy rate of 10.6% but by 1988 this had risen to 25.6% he claimed that illegitimate children are more likely to come from women of the lower class and that they run wild due to the lack of a father figure and in effect he held them responsible for rising crime, property crime and violent crime. This in turn damaging communities making the residential area deprived with little amenities and also made people withdraw into themselves causing all kinds of illnesses mainly psychological. A critic of this is that there is no evidence to prove his conclusions and there are no significant differences between the lower class and the employed in their attitudes towards work and it can be seen that mothers with husbands/fathers spend more time claiming benefits than single mothers. Naidoo and wills (2000) suggests that the Marxist approach to poverty and unemployment ties in with the social scientists perspective on medicine, as they argue that medicine is closely linked to power and is still a powerful means of social control, as without medicine health would deteriorate and society would lack structure. [LF6]
There are many medical models that look at the determinants of health. The behaviour change model aims to encourage individuals to adapt healthy behaviours which are seen as the key to improve health and wellbeing. It can be argued as this model does not reflect the understanding of poverty the approach is popular as it views health as a property of individuals, making it possible to assume that people can change their behaviours to make improvements to their health. It also states that individuals who do not care for themselves are to blame for the consequences of ill health.
When looking at poverty and unemployment and this approach it is impossible to change behaviours and lifestyles for improved health when they are outside the individuals control, there has to be some amount of flexibility to be able to make changes, individuals living in poverty and who are unemployed know that changing bad lifestyles is not always as easy as it may seem.

The above shows how the Behaviour change model works.
On the other hand a health model that can be tied in with poverty is the Social change model the main aim of this approach is to enable people to gain control of their lives, it enables people to gain skills and confidence, and empowerment is also used as a way to describe a way of working which increases peoples power to change their social reality, an example of this in communities there are self-help groups and community based development like setting goals and community based development such as meeting in order to meet specific needs like clean-up programmes and such, this would help individuals in poverty and unemployment gain confidence to learn new skills in order to find a job which in turn would improve their health or even help individuals with depression or stress by meeting new people going through the same thing. [LF7]

The picture above shows the different stages of the social change model.
This approach also attempts to bring changes in the physical, social and economic environment this includes things like bans in public places for example smoking, which in turn will decrease or attempt to decrease smoking levels in more deprived areas which could result in saving money and starting the long road out of poverty. It can also be suggested that it could reduce air pollution as if the area of residence has high air pollution then this carries a more detrimental issue on health in regards to individuals who are medically unwell or have illnesses such as asthma or emphysema.
Air pollution is a major environmental risk to health. By reducing air pollution levels, countries can reduce the burden of disease from stroke, heart disease, lung cancer, and both chronic and acute respiratory diseases, including asthma. The lower the levels of air pollution, the better the cardiovascular and respiratory health of the population will be, both long- and short-term. The “WHO Air quality guidelines” provide an assessment of health effects of air pollution and thresholds for health-harmful pollution levels.
Ambient (outdoor air pollution) in both cities and rural areas was estimated to cause 3.7 million premature deaths worldwide in 2012. [LF8]
Some 88% of those premature deaths occurred in low- and middle-income countries, and the greatest number in the WHO Western Pacific and South-East Asia regions. Policies and investments supporting cleaner transport, energy-efficient housing, power generation, industry and better municipal waste management would reduce key sources of urban outdoor air pollution. Reducing outdoor emissions from household coal and biomass energy systems, agricultural waste incineration, forest fires and certain agro-forestry activities (e.g. charcoal production) would reduce key rural and peri-urban air pollution sources in developing regions. Reducing outdoor air pollution also reduces emissions of CO2 and short-lived climate pollutants such as black carbon particles and methane, thus contributing to the near- and long-term mitigation of climate change. In addition to outdoor air pollution, indoor smoke is a serious health risk for some 3 billion people who cook and heat their homes with biomass fuels and coal (WHO, 2014)
Very good discussion with clear evaluation of theories and models.
Conclusion
In conclusion, it can be seen that poverty is the main cause to ill health within society, regardless of age, ethnicity, religion, social class. It all comes down to poverty, as without the means to live a healthy lifestyle, individuals cannot change behaviours and attitudes towards healthier living. Poverty can cause disease and illness and affect general health through stress. Psychologically becoming depressed over money worries, poor living conditions and lack of nutrition or too much junk food and alcohol can cause obesity, diabetes and liver damage. If the area is industrial or run down an individual has more change[LF9] of developing lung disease and breathing difficulties.
Poverty is a term which is defined as very wide spread and there are millions of implications to health and what living in poverty can cause.
A very good report which discusses models, theories, concepts and issues well. To further improve:
- Make sure you ‘un-pick’ a concept thoroughly in order to give a greater level of evaluation.
- Take care with referencing – you need to review this practise (study skills handout and/or Cite Them Right)
- Make sure the sections of your report are clearly defined by way of section headings.
Table of References
Butterfield, W.J.H. (1968) ‘priorities in medicine’. London: Nuffield
Naidoo, J. & Wills, J. (2000) ‘Health promotion’ (2nd edition) London: Bailliere Tindal
Ogden, J. (1996) ‘Health psychology’ Buckingham: University press
Katz, J., Peberdy, A. (1997) ‘Promoting health, knowledge and practise’ Basingstoke: Open University press.
World Health Organisation. (2014) ‘Ambient air quality and health’ [online] Available at: < http://www.who.int/mediacentre/factsheets/fs313/en/> [Accessed – 5th May 2014]
Very good sources.
Kirsty Lincoln
[LF1]If this were an essay this would be allowed therefore this should have been a Report! Also I can’t identify where your Introduction ends and Discussion of Findings starts etc.
[LF2]Capital Letter
[LF3]It is important here to point out that you are basing this upon US statistics.
[LF4]Source?
[LF5]Source?
[LF6]Good points made and evaluated here.
[LF7]Very good discussion of models however where are you getting your information from??
[LF8]Sources??
[LF9]‘chance’
Cite This Work
To export a reference to this article please select a referencing stye below:
Related Services
View all


DMCA / Removal Request
If you are the original writer of this essay and no longer wish to have your work published on UKEssays.com then please click the following link to email our support team:
Request essay removal